
Written by Jill Ashey
Edited by Bobbie Renfro
Just like us, corals can get sick. Unfortunately, unlike us, corals can’t visit the doctor to help them get better. Stony coral tissue loss disease (SCTLD) has become a prevalent and deadly coral disease in the Florida Keys and Caribbean. This disease quickly kills coral colonies, as it eats away at coral tissue and exposes patches of white skeleton. Since its discovery in 2014 off the coast of Miami, Florida, SCTLD has spread rapidly, devastating reefs throughout the Caribbean. Many coral species are highly susceptible to this disease and die within weeks to months of infection. SCTLD’s rapid spread and high mortality rate have generated a plethora of SCTLD-focused research, but the transmission method and cause of the disease is unknown.
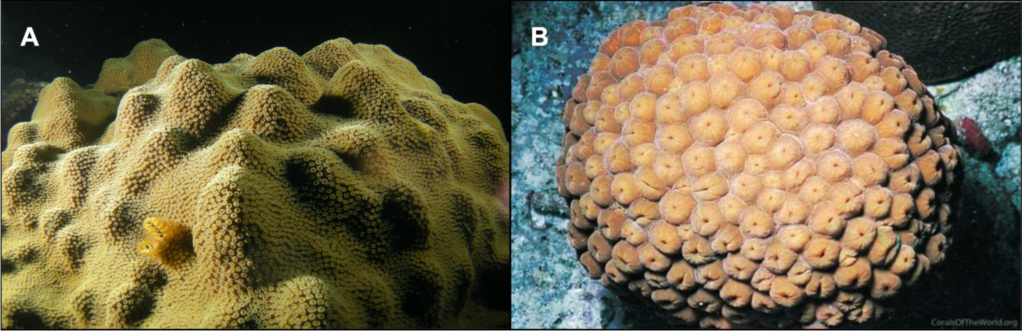
To address these questions, Studivan et al. (2022) investigated if reef sediment could be “infected” with SCTLD and if that infected sediment could transmit the disease to corals. Additionally, they examined the microbes in the infected sediment to explore the connections between microbial communities and coral disease. For their experiment, they used the coral species the great star coral, Montastraea cavernosa, and the mountainous star coral, Orbicella faveolata (Figure 1). Both species are prominent reef builders in the Caribbean and have shown high susceptibility to SCTLD.
Experimental design
To evaluate sediment as a possible vector for SCTLD, researchers exposed coral fragments to one of four treatments (Figure 2):
- (1) healthy sediment – healthy corals placed on sediment never exposed to diseased corals
- (2) disease contact – healthy corals placed in direct contact with other diseased corals on top of healthy sediment
- (3) batch diseased sediment – healthy corals placed on sediment infected by exposure to a diseased M. cavernosa colony
- (4) individual diseased sediment – healthy corals placed on sediments infected by diseased coral fragments obtained from the disease contact treatment.

The sediment was infected in two different ways (batch and individual) in order to better understand the ability of sediment at transmitting disease alone. During the exposures, the corals were monitored daily by researchers, who measured the time to infection, as well as signs of infection (lesions, tissue loss, whitening of tissue, etc). Once the characteristic SCTLD lesions were observed in at least 50% of the corals exposed, corals and sediments from each treatment were collected and preserved.
To characterize the microbial community composition in the sediment, DNA from the microbes in the sediment samples was extracted. Researchers then amplified and sequenced the 16S rRNA gene. The 16S rRNA gene codes for the small subunit of the ribosome, a cellular structure. This gene code is present in all bacteria and archaea. The use of this ubiquitous gene allows 16S rRNA information from all microbe species in a sample to be captured, amplified, and sequenced. Additionally, parts of the 16S rRNA gene are species-specific, making it easy to differentiate between closely related species detected in a sample.
What did they find?
The study found that sediment can indeed act as a vector spreading SCTLD in M. cavernosa and O. faveolata. The highest rates of transmission occurred in the disease contact treatments, but substantial transmission was observed in the sediment treatments. In both sediment treatments (batch and individual), more than 65% of M. cavernosa corals were infected. O. faveolata, on the other hand, had only 33% of corals infected in both sediment treatments; the lower transmission rate in O. faveolata may be because the original disease colony was M. cavernosa, a different species. In the disease contact treatment and the batch sediment treatment, it took several days to a week for corals to become infected. However, in the individual sediment treatment, it took ~24 hours for both species of coral to become infected, suggesting that sediment inoculation time may have some impact on the infectioness of SCTLD.
Many different kinds of microbes were found in the sediment samples, and there were different microbes in the different treatments. Several microbial genera, such as Porticoccus, Pelagibus, and Magnetopsira, were identified in SCTLD-infected corals experiencing tissue loss. These genera have been implicated in other coral diseases, such as white plague disease type II, white band disease, and black band disease (Sunagawa et al. 2009; Miller & Richardson 2011; Gignoux-Wolfsohn et al. 2020). The Vibrio genus was also observed in SCTLD-infected corals experiencing tissue loss, which has been enriched in tissue lesions in prior studies (Meyer et al. 2019; Ushijima et al. 2020). These results suggest that these specific microbial players could act as indicators for coral disease and/or SCTLD.
What does this mean?
Knowing that reef sediment may be spreading SCTLD helps us understand how the disease may be transmitted and hopefully can help us figure out how to prevent further spread. Coastal development in Florida and several Caribbean islands has resulted in increased dredging, causing sedimentation and murky water on many reefs. It is possible that the suspended sediment generated from these activities is transported to other reefs via currents or human movement of sediment, suggesting that sediment may be an important component of SCTLD spread. In order to contain this disease, it is imperative to manage further coastal development projects that could disrupt sediment near reefs.
This work also provides a stepping stone into characterizing the microbes involved in SCTLD. By knowing the microorganisms that are present in SCTLD infection, researchers can better predict and mitigate the effects of this disease. Additionally, the characterization of the microbial community can enhance efforts to create a treatment that will prevent or slow this disease. Maybe corals will be able to go to the doctor someday!
Citations
Featured image: M. Brandt, https://www.sciencenews.org/article/mysterious-coral-disease-ravaging-caribbean-reefs
Paper: Studivan MS, Rossin AM, Rubin E, Soderberg N, Holstein DM and Enochs C. 2022. Reef sediments can act as a stony coral tissue loss disease vector. Frontiers in Marine Science. 8:815698. doi: 20.3389/fmars.2021.815698
Gignoux-Wolfsohn, S.A., Precht, W.F., Peters, E.C., Gintert, B.E., & Kaufman, L.S. (2020). Ecology, histopathology, and microbial ecology of a white-band disease outbreak in the threatened staghorn coral Acropora cervicornis. Diseases of Aquatic Organisms. 137,217-237. https://doi.org/10/3354/dao03441
Meyer, J.L., Fastellanos-Gell, J., Aeby, G.S., Häse, C.C., Ushijima, B., & Paul, V.J. (2019). Microbial community shifts associated with the ongoing stony coral tissue loss disease outbreak on the Florida Reef Tract. 10,2244. https://doi.org/10.3389/fmicb.2019.02244
Miller, A.W. & Richardson, L.L. (2011). A meta-analysis of 16S rRNA gene clone libraries from the polymicrobial black band disease of corals. FEMS Microbiology Ecology. 75(2), 231-241. https://doi.org/10.1111/j.1574-6941.2010.00991.x
Sunagawa, S, DeSantis, T.Z., Piceno, Y.M., Brodie, E.L., DeSalvo, M.K., Voolstra, C.R., Weil, E., Anderson, G.L., & Medina, M. (2009). Bacterial diversity and White Plague Disease-associated community changes in the Caribbean coral Montastraea faveolata. The ISME Journal. 3,512-521. https://doi.org/10.1038/ismej.2008.131
Ushijima, B., Meyer, J.L., Thompson, S., Pitts, K., Marusich, M.F., Tittl, J., Weatherup, E., Reu, J., Wetzell, R., Aeby, G.S., Häse, C.C., & Paul, V.J. (2020). Disease diagnostics and potential coinfections by Vibrio coralliilyticus during an ongoing coral disease outbreak in Florida. Frontiers in Microbiology. 11,2682. https://doi.org/10.3389/fmicb.2020.569354
