
Written by Sara GAGLIARDI
Edited by Brad WEILER
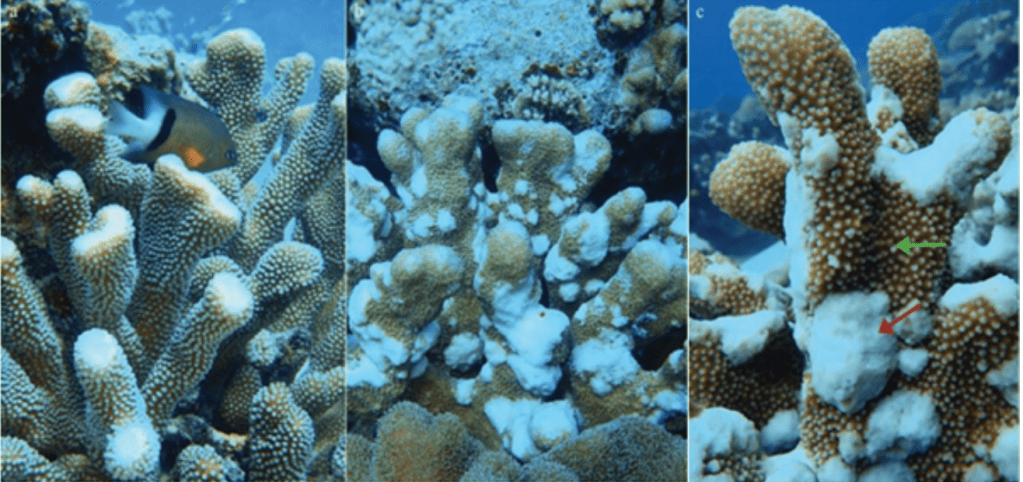
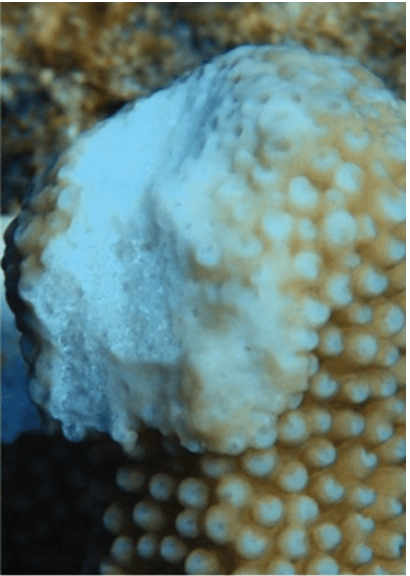
Just as humans and other animals (e.g., dogs1), scleractinian corals can be affected by a tumour-like disease called growth anomalies (GAs). Growth anomalies are characterised by abnormal skeletal growths forming pale protuberant masses with undulating margins and nodular relief that change the shape of corals (Fig. 1), and have been documented worldwide, from the Caribbean and Western Atlantic, to the Indo-Pacific and Red Sea 2,3. They affect 14 genera, with Acropora and Porites being the most concerned4, and disturb the feeding, defences and reproduction processes of corals, which are critical biological functions for their survival. Even though the negative impacts of GAs on the coral host have been well described, the pathology –transmission and causality– of the disease remains unknown. However, the prevalence of GAs was linked to the human population size, and sea surface temperature and ultraviolet radiation anomalies4.
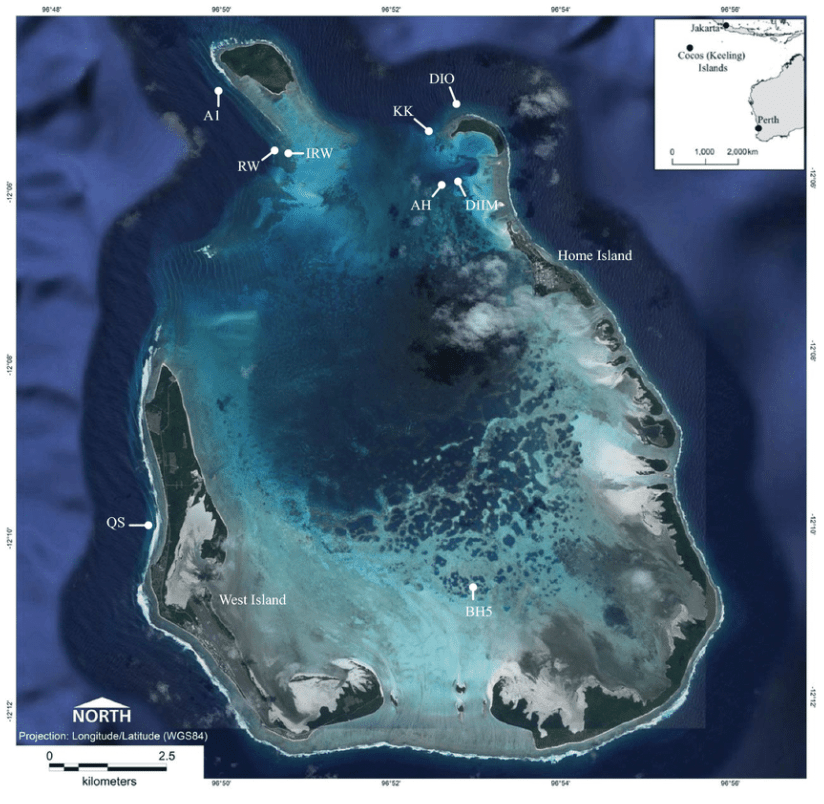
In their research2 in Cocos (Keeling) Islands (CKI), East Indian Ocean, Sophie Preston and Dr. Zoe Richards addressed the extent of GAs in the region. The researchers selected 9 collection sites (Fig. 2) and focused on the species Isopora palifera, a scleractinian, reef-building coral that is supposed to have suffered an outbreak of GAs in 2018.
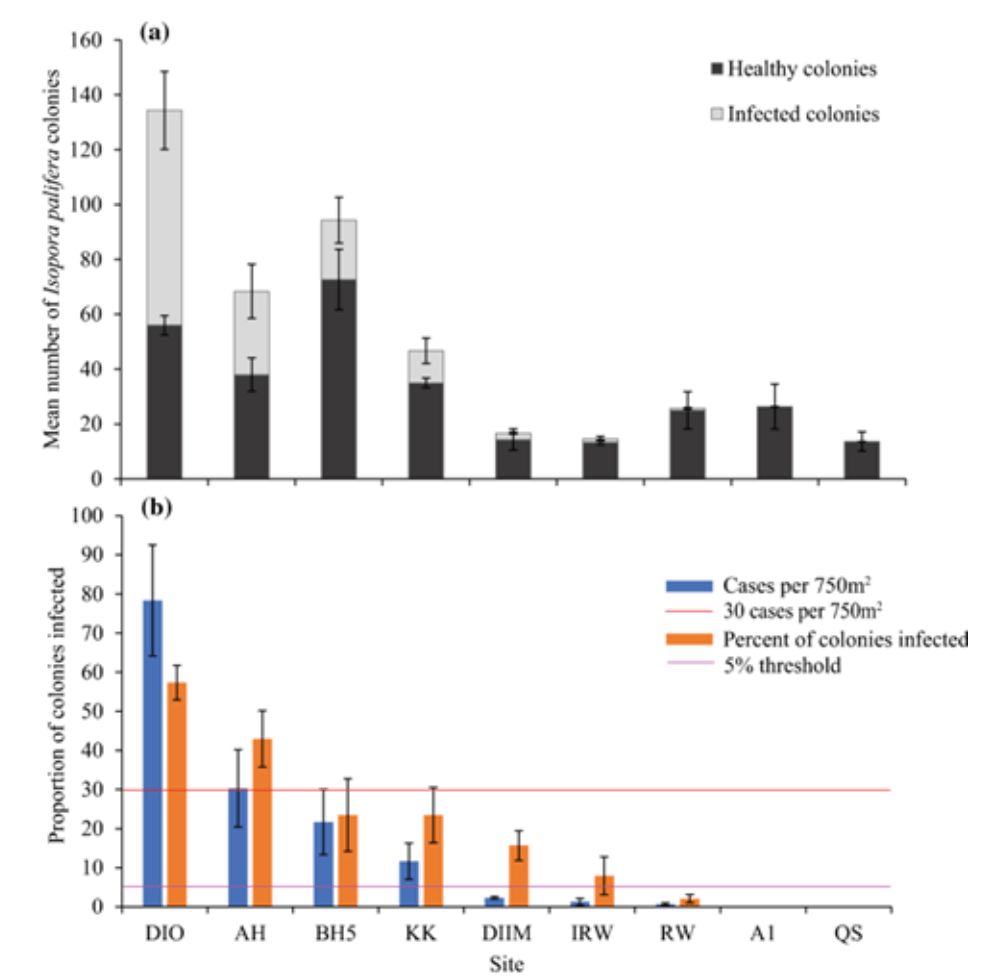
To explore whether the occurrence of GAs among the coral populations in the region could be classified as an outbreak, they surveyed two ecological aspects: the coral distribution and abundance in the reef, and the proportion of diseased specimens. The disease outbreak was assigned following Willis et al.5, who qualifies an outbreak when more than 5% of corals are diseased, and Maynard et al.6, who qualifies an outbreak when more than 30 cases per 750 m2 are present.
Results showed that I. palifera accounted for approximately 6% of the total hard coral cover (the sixth most prevalent species), however large differences in mean number of colonies between sites were observed (Fig. 3). All sites presented infected colonies, except for two sites that also showed the lower number of coral colonies. Overall, 33% of the colonies were infected with GAs. More specifically, the proportion of the population showing symptoms of disease was higher than 5% in six of nine sites, whereas only two sites presented more than 30 cases per 750 m2 (DIO with 78.33 and AH with 30.33, respectively). Hence, CKI is experiencing an outbreak of GAs. It was therefore important to establish how the disease influences the growth and viability of the coral population in the region.
To study the effects that GAs have on the fecundity and growth, skeletal deposition, and tissue degradation of I. palifera, researchers carried out two procedures. First, they tested the differences in trace element composition of healthy and infected skeletons, as the symptoms of the disease are related to skeletal growth. Corals were subjected to X-ray fluorescence analysis, a real-time, non-destructive testing that allows to detect the presence and concentration of metals in a sample.
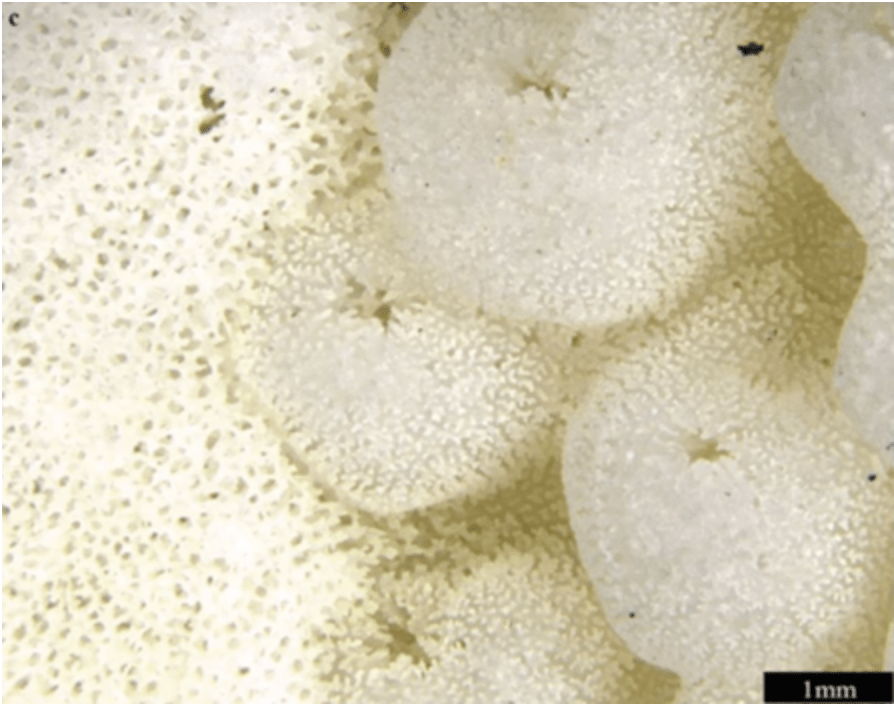
The evaluation showed that the chemical composition differed according to the site and health status of the colony. These differences suggest a shift in the crystal structure of the aragonite (healthy samples) forming the skeleton to the less dense calcite (infected samples), that results in a loss of structure and an increase in porosity (Fig. 4). Moreover, bacteria may consume the calcite (bioerosion) and create an anoxic “marine cement” on the coral colony. Therefore, the progress of GAs may be due to both environmental (relation to the site) and microbial (bioerosion) factors.
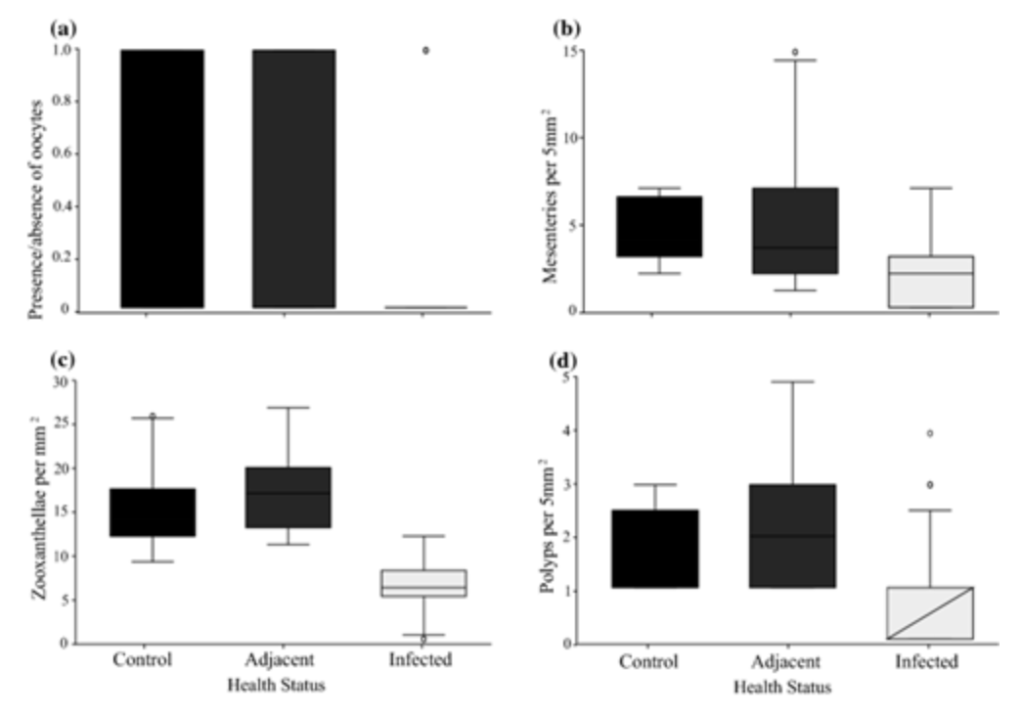
Secondly, they observed the histological structure of corals – one healthy (control), one infected and one adjacent healthy tissue per sample – through microscopy to measure the reproductive and biological functioning of the tissues. Hence, they observed the presence/absence of oocytes, the density of zooxanthellae, and the number of polyps and mesenteries – i.e., the internal, longitudinal tissue that provides the coral structural support and increasing surface, allowing a better nutrition and fertility.
As it was predicted, the density of oocytes, mesenteries, polyps, and zooxanthellae was significantly lower in diseased tissues. More specifically, oocytes were present in only one sample. Therefore, based on the coral cover and the proportion of infected colonies, the decrease of the reproductive potential of I. palifera could threaten the success of the CKI reef and the conservation of associated taxa. However, Acropora and Porites, the most GA-affected genera, were disproportionately touched by the disease despite their major presence in the reef and the direct contact with infected colonies. This opens the question whether GAs transmission is indiscriminately or is specific to the coral species.
It was also observed that fish might have an important role for the clean-up of the disease lesion, as they preferentially feed upon it (predatory mechanism, Fig. 6). However, further studies are needed to determine the extent of their role in GA dynamics.
In conclusion, it is likely the outbreak of GAs is due to a complex combination of environmental, anthropogenic, microbial, and predatory factors, which makes it difficult for researchers to determine the exact reasons and mechanisms that establish and extend the disease. However, new techniques are rising from the biomedical and veterinary sciences, providing concepts, tools, and methodologies for the investigation of coral diseases7. Complimenting and improving previously established biomedical methodologies gives us hope in the ability to uncover coral pathogens, slowing their impact on coral reefs globally through direct intervention by coral reef conservationists, researchers, and local managers.
References
1. Brønden, L. B., Flagstad, A. & Kristensen, A. T. Veterinary cancer registries in companion animal cancer: a review. Veterinary and Comparative Oncology 5, 133–144 (2007).
2. Preston, S. & Richards, Z. Biological consequences of an outbreak of growth anomalies on Isopora palifera at the Cocos (Keeling) Islands. Coral Reefs 40, 97–109 (2021).
3. Mohamed, A. R. & Sweet, M. Current Knowledge of Coral Diseases Present Within the Red Sea. in Oceanographic and Biological Aspects of the Red Sea (eds. Rasul, N. M. A. & Stewart, I. C. F.) 387–400 (Springer International Publishing, 2019). doi:10.1007/978-3-319-99417-8_21.
4. Aeby, G. S. et al. Growth Anomalies on the Coral Genera Acropora and Porites Are Strongly Associated with Host Density and Human Population Size across the Indo-Pacific. PLOS ONE 6, e16887 (2011).
5. Willis, B. L., Page, C. A. & Dinsdale, E. A. Coral Disease on the Great Barrier Reef. in Coral Health and Disease (eds. Rosenberg, E. & Loya, Y.) 69–104 (Springer, 2004). doi:10.1007/978-3-662-06414-6_3.
6. Maynard, J. A. et al. Predicting outbreaks of a climate-driven coral disease in the Great Barrier Reef. Coral Reefs 30, 485–495 (2011).
7. Work, T. M., Richardson, L. L., Reynolds, T. L. & Willis, B. L. Biomedical and veterinary science can increase our understanding of coral disease. Journal of Experimental Marine Biology and Ecology 362, 63–70 (2008).
Cover Photo courtesy of Coral Health Atlas.
